Q. What is Prostate Gland?
A. Prostate is a gland about the size of a walnut that is present only in men. It is located just below the bladder and surrounds the urethra, the tube through which urine flows from the bladder and out through the penis. One of the main functions of the prostate gland is to produce prostatic fluid, one of the components of semen. A man's prostate gland usually starts to enlarge after he reaches 40 years of age. This condition is called benign prostatic hyperplasia (BPH). It is not cancer, and it does not raise your risk for prostate cancer.
Prostate is a gland about the size of a walnut that is present only in men. It is located just below the bladder and surrounds the urethra, the tube through which urine flows from the bladder and out through the penis. One of the main functions of the prostate gland is to produce prostatic fluid, one of the components of semen. A man's prostate gland usually starts to enlarge after he reaches 40 years of age. This condition is called benign prostatic hyperplasia (BPH). It is not cancer, and it does not raise your risk for prostate cancer.
 Once prostate growth starts, it often continues, unless medical therapy is started. Prostate grows in two different ways. In the first type of growth, cells multiply around the urethra and squeeze it, much like you can squeeze a straw. The second type of growth is the middle-lobe prostate growth, in which cells grow into the urethra and the bladder outlet area.
Once prostate growth starts, it often continues, unless medical therapy is started. Prostate grows in two different ways. In the first type of growth, cells multiply around the urethra and squeeze it, much like you can squeeze a straw. The second type of growth is the middle-lobe prostate growth, in which cells grow into the urethra and the bladder outlet area.
Q. What is Benign Prostatic Hyperplasia: A common part of aging
A. It is common for the prostate gland to become enlarged as a man ages. Doctors call this condition benign prostatic hyperplasia (BPH), or benign prostatic hypertrophy.
As a man matures, the prostate goes through two main periods of growth. The first occurs early in puberty, when the prostate doubles in size. At around age 25, the gland begins to grow again. This second growth phase often results, years later, in BPH.
Though the prostate continues to grow during most of a man's life, the enlargement doesn't usually cause problems until late in life. BPH rarely causes symptoms before age 40, but more than half of men in their sixties and as many as 90 percent in their seventies and eighties have some symptoms of BPH.
With obstruction, the bladder wall becomes thicker and irritable. The bladder begins to contract even when it contains small amounts of urine, causing more frequent urination. Eventually, the bladder weakens and loses the ability to empty itself, so some of the urine remains in the bladder. The narrowing of the urethra and partial emptying of the bladder cause many of the problems associated with BPH.
Many people feel uncomfortable talking about the prostate, since the gland plays a role in both sex and urination. Still, prostate enlargement is as common part of aging as gray hair. As life expectancy rises, so does the occurrence of BPH.
Q. Why BPH (Benign Prostatic Hyperplasia) Occurs
A. The cause of BPH is not well understood. No definite information on risk factors exists. For centuries, it has been known that BPH occurs mainly in older men and that it doesn't develop in men whose testes were removed before puberty. For this reason, some researchers believe that factors related to aging and testicular hormones may spur the development of BPH.
Q. What are the symptoms of enlarged prostate?
A. The most common ones involve changes or problems with urination, such as
The size of the prostate does not always determine how severe the obstruction or the symptoms will be. Some men with greatly enlarged glands have little obstruction and few symptoms while others, whose glands are less enlarged, have more blockage and greater problems.
Q. How can enlarge prostate be diagnosed?
A. You may first notice symptoms of BPH yourself, or your doctor may find that your prostate is enlarged during a routine checkup. When BPH is suspected, you may be referred to a doctor who specializes in problems of the urinary tract and the male reproductive system. Several tests help the doctor identify the problem and decide whether surgery is needed. The tests vary from patient to patient, but the following are the most common.
Digital Rectal Examination (DRE): - This examination is usually the first test done. The doctor inserts a gloved finger into the rectum and feels the part of the prostate next to the rectum. This examination gives the doctor a general idea of the size and condition of the gland.
Prostate-Specific Antigen (PSA) Blood Test: - To rule out infection or cancer as a cause of urinary symptoms, your doctor may recommend a PSA blood test. PSA, a protein produced by prostate cells, is frequently present at elevated levels in the blood of men who have prostate infection or cancer.
Transabdominal / Transrectal Ultrasound: - It shows the size and weight of prostate for further evaluation.
Prostate Biopsy: - The doctor can use the probe and the transrectal ultrasound images to guide a biopsy needle to the suspected area. The needle collects a few pieces of prostate tissue for examination with a microscope.
Urine Flow Study: - Your doctor may ask you to urinate into a special device that measures how quickly the urine is flowing. A reduced flow often suggests BPH.
Q. What is the treatment option of Enlarged Prostate?
A. Drug Treatment Over the years, researchers have tried to find a way to shrink or at least stop the growth of the prostate without using surgery. These drugs may work on some patient but not at all work on other patients.
The latest Non-Surgical treatment for Enlarged Prostate, the technique called: - Prostatic Artery Embolization (PAE) Now a new procedure has been developed that is comparable to TURP in recovery of the symptoms.
In this procedure the patient stops all prostatic medication before embolization, Only few medicines related to the procedure are given for 10-12 days.after the procedure. The patients are admitted to the hospital on the day of the procedure. During embolization, pain medication, anti-inflammatory drugs and antibiotic are given.
 Prostatic Artery Embolization
Prostatic Artery Embolization
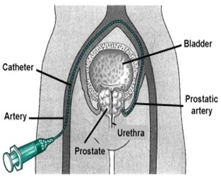
Embolization is performed under local anesthesia by unilateral approach, usually the right femoral artery. Initially, pelvic angiography is performed to evaluate the iliac and prostatic arteries. Then, a 4 or 5-F angiography catheter is introduced in right femoral artery to catheterize the Prostatic artery and finally the prostatic vessels are selectively catheterized with a 3-F coaxial microcatheter. The angiography study is performed to confirm the position of the catheter in the ostium of the prostatic artery before embolization. For embolization, PVA particles were used. The endpoint chosen for embolization was slow flow or near-stasis in the prostatic vessels with interruption of the arterial flow and prostatic gland opacification.
 Traditional Surgical Treatment
Traditional Surgical Treatment
Most doctors recommend removal of the enlarged part of the prostate as the best long-term solution for patients with BPH. With surgery for BPH, only the enlarged tissue that is pressing against the urethra is removed; the rest of the inside tissue and the outside capsule are left intact. Surgery usually relieves the obstruction and incomplete emptying caused by BPH. The following section describes the types of surgery that are used.
Transurethral surgery: - In this type of surgery, no external incision is needed. After giving anesthesia, the surgeon reaches the prostate by inserting an instrument through the penis. A procedure called transurethral resection of the prostate (TURP) is used for 90 percent of all prostate surgeries done for BPH. With TURP, an instrument called a resectoscope is inserted through the penis. The resectoscope, which is about 12 inches long and 1/2 inch in diameter, contains light valves for controlling irrigating fluid, and an electrical loop that cuts tissue and seals blood vessels. During the 90-minute operation, the surgeon uses the resectoscope's wire loop to remove the obstructing tissue one piece at a time. The pieces of tissue are carried by the fluid into the bladder and then flushed out at the end of the operation.
Most doctors suggest using TURP whenever possible. Transurethral procedures are traumatic forms of surgery. One possible side effect of TURP is retrograde, or backward, ejaculation. In this condition, semen flows backward into the bladder during climax instead of out the urethra.
Open surgery: - In the few cases when a transurethral procedure cannot be used, open surgery, which requires an external incision, may be used. Open surgery is often done when the gland is greatly enlarged, when there are complicating factors, or when the bladder has been damaged and needs to be repaired. The location of the enlargement within the gland and the patient's general health help the surgeon decide which of the three open procedures to use. With all the open procedures, anesthesia is given and an incision is made. Once the surgeon reaches the prostate capsule, he or she scoops out the enlarged tissue from inside the gland.
Q. Is Prostatic Artery Embolization (non-surgical treatment) a safe procedure?
A. Prostatic artery embolization has been performed safely in thousands of mans worldwide. While no procedure is without risk, prostate embolization has been shown to have a lower complication rate than traditional surgical treatment options such as surgery. The few complications are like failure rate is about 1-2%.
Q. What can I expect during the procedure?
A. PAE requires an overnight or day stay in hospital. Prior to embolization, the patient will be catherized for 4-6 hrs. Most procedures take approximately 20-30 minutes. An Interventional Radiologist performs the PAE through a small catheter inserted into the femoral artery in the groin. A local anesthetic is used to numb the skin and no stitches are needed after the procedure.
An X-ray is performed to give the doctor a clear picture of the blood supply to the prostate using angiographic techniques, the catheter is guided through the artery to the prostate and tiny plastic particles are slowly injected into the arteries that supply blood to the enlarged prostate. Over several minutes, these particles block the blood supply to the prostate. With-out a blood supply, an enlarged prostate will shrink up to 40-50% in 1st 4-5 weeks. The embolization is continued until the blockage of blood flow to the prostate is complete. After complete embolization of one side is done, the other side is embolized.
Q. What happens to the Prostate after Prostatic Artery Embolization?
A. After PAE, the prostate shrink and patient get relief from symptoms of enlarged prostate.
Q. Any size of enlarged Prostate that cannot be treated with PAE?
A. Yes any size of the enlarge prostate can be successfully treated by PAE. If the size is more than 45 gm they get the good results.
Q. What are advantages of Prostatic Artery Embolization ( PAE)
Q. Do prostate grow back after PAE?
A. There is no evidence at this time that adequately treated enlarged prostate grows back after prostatic artery embolization.
Q. Will my insurance cover Prostatic Artery Embolization?
A. Most major insurance companies are now covering uterine fibroid embolization. Depending on your plan, specific referrals or other preauthorization may be necessary. Our clinical coordinator will assist you thru the approval process.
A. The Prostatic Artery Embolization procedure itself is painless. It is done under local anesthetic shot at the puncture site near the right hip. For the mild pain reason, we keep patients overnight in the hospital for pain control.
Q. How long until I can return to work after PAE?
A. The average recovery time before patients return to work or their normal daily activities is approximately one to three days. On next day you can resume the normal activity.
Q. What type of follow-up is required after the PAE procedure?
A. After the procedure, we ask you to return to our office for routine follow-up in 2-3 days. We also ask that you schedule an appointment to see your gynecologist in two to three months after the procedure for a routine gynecologic exam. We will plan for follow-up MRI in six to nine months to assess the results of embolization and to insure that the blood supply to the fibroids is eliminated.
A. While it varies significantly from country to country and hospital to hospital, in general, Prostatic Artery Embolization is less expensive to TURP / laser and other prostate surgery. In many areas, it is reported to be less expensive due to the shorter hospital stay and no need for general anesthesia.
Q. How successful is PAE in controlling symptoms caused by enlarged prostate?
A. The symptoms are controlled in 95-97 percent of patients after their procedure. Bulk related symptoms such as increased urination, hesitation to urinate, sexual dysfunction, and retrograde ejaculation are controlled in 95-98 percent of patients undergoing PAE. The 2-3% of the patient may not get the symptom relief.